- Spinal Cord Injury An introduction for people new to spinal cord injury
- What is spinal cord injury Understanding the essence of spinal cord injury
- Understanding spinal cord injury Where is the injury? C4, C6 . . .
- Injury, effects and impacts Injuries to the spine have effects on the nervous system that lead to impacts in people's lives
- Rehabilitation The rehabilitation process from injury to living in the community
- Adjusting to spinal cord injury People's experiences of having spinal cord injury
- Attendant care challenges Challenges for people with spinal cord injury receiving attendant care
Understanding spinal cord injury
What is the spinal column?
The spinal column (or spine) is a structure made up of bones (vertebrae), nerves and ligaments. It provides support for the body and protects the spinal cord.
There are 33 vertebrae running from the base of the skull to the tailbone. They are stacked and held together by disks, ligaments and muscles.
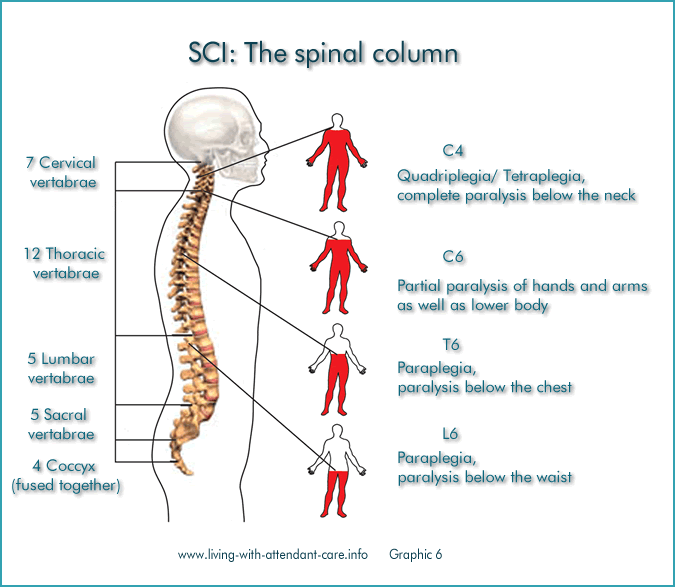
The spinal column is classed in sections with each vertebra being numbered. There are:
- 7 cervical vertebrae in the neck
- 12 thoracic vertebrae in the upper back
- 5 lumbar vertebrae in the lower back
- 5 sacral vertebrae that are joined to form the sacrum and
- 4 coccygeal vertebrae that are fused to form the coccyx
Each vertebra is referred to by its name and number, so that the cervical vertebrae are called C1 to C7 with the numbers counting downwards from the head. So the thoracic vertebrae become T1 – T12, and the lumbar vertebrae L1 – L5.
The location of the injury determines what part of the body is impacted. For example an injury at C4 causes complete paralysis below the neck, whereas an injury at L6 causes paralysis below the waist.
ParaquadWhat is the spinal cord?
The spinal cord allows your brain to communicate with your body by sending “messages” through the nerves.
The spinal cord runs from your brain down the inside of your spinal column and is made up of millions of nerve fibres. At each vertebra, nerves branch out to send and receive information to and from different parts of the body. Both the nerves and the vertebra are numbered in the same way.
Messages are sent from the brain down the spinal cord to control every function of the body, some of which are under our control (the Somatic Nervous System) and others happen without us knowing (the Autonomic Nervous System). By controlling automatic, involuntary functions,
the autonomic nervous system’s main function is maintaining a stable environment within the body.
Some functions include blood flow, heart function, breathing, body temperature and some aspects of bladder and bowel function.
If you have damaged your spinal cord you have probably damaged your autonomic nervous system.
Functional goals
It is useful to consider what can be realistically achieved by a person with SCI for any particular injury location.
Functional goals are a realistic expectation of activities that a person with spinal cord injury eventually should be able to do with a particular level of injury.
These goals are set during rehabilitation with the medical team. They help the
individual with SCI learn new ways to manage his/ her daily activities and stay healthy.
Achievement of functional goals can also be affected by other factors, such as an individual’s body type and health related issues. By striving to reach these functional goals, the hope is to give individuals with SCI the opportunity to achieve MAXIMUM INDEPENDENCE.
The chart,Functional Goals for Specific Levels of Complete Injury, shows the expected functional goals for a person with a complete injury at a particular level. Motor and sensory functions improve with lower levels of injury.
Spinal Cord Injury - Functional Goals for Specific Levels of Complete Injury |
||
Level |
Abilities |
Functional Goals |
| C1-C3 | C3-limited movement of head and neck | Breathing: Depends on a ventilator for breathing. Communication: Talking is sometimes difficult, very limited or impossible. If ability to talk is limited, communication can be accomplished independently with a mouth stick and assistive technologies like a computer for speech or typing. Effective verbal communication allows the individual with SCI to direct caregivers in the person’s daily activities, like bathing, dressing, personal hygiene, transferring as well as bladder and bowel management. Daily tasks: Assistive technology allows for independence in tasks such as turning pages, using a telephone and operating lights and appliances. Mobility: Can operate an electric wheelchair by using a head control, mouth stick, or chin control. A power tilt wheelchair also for independent pressure relief. |
| C3-C4 | Usually has head and neck control. Individuals at C4 level may shrug their shoulders. |
Breathing: May initially require a ventilator for breathing, usually adjust to breathing full-time without ventilatory assistance. Communication: Normal. Daily tasks: With specialized equipment, some may have limited independence in feeding and independently operate an adjustable bed with an adapted controller. |
| C5 | Typically has head and neck control, can shrug shoulder and has shoulder control. Can bend his/her elbows and turn palms face up. |
Daily tasks: Independence with eating, drinking, face washing, brushing of teeth, face shaving and hair care after assistance in setting up specialized equipment Health care: Can manage their own health care by doing self-assist coughs and pressure reliefs by leaning forward or side -to-side. Mobility: May have strength to push a manual wheelchair for short distances over smooth surfaces. A power wheelchair with hand controls is typically used for daily activities. Driving may be possible after being evaluated by a qualified professional to determine special equipment needs |
| C6 | Has movement in head, neck, shoulders, arms and wrists. Can shrug shoulders, bend elbows, turn palms up and down and extend wrists |
Daily tasks: With help of some specialized equipment, can perform with greater ease and independence, daily tasks of feeding, bathing, grooming, personal hygiene and dressing. May independently perform light housekeeping duties. Health care: Can independently do pressure reliefs, skin checks and turn in bed. Mobility: Some individuals can independently do transfers but often require a sliding board. Can use a manual wheelchair for daily activities but may use power wheelchair for greater ease of independence. |
| C7 | Has similar movement as an individual with C6, with added ability to straighten his/her elbows. |
Daily tasks: Able to perform household duties. Need fewer adaptive aids in independent living. Health care: Able to do wheelchair pushups for pressure reliefs. Mobility: Daily use of manual wheelchair. Can transfer with greater ease. |
| C8-T1 | Has added strength and precision of fingers that result in limited or natural hand function. |
Daily tasks: Can live independently without assistive devices in feeding, bathing, grooming, oral and facial hygiene, dressing, bladder management and bowel management. Mobility: Uses manual wheelchair. Can transfer independently. |
| T2-T6 | Has normal motor function in head, neck, shoulders, arms, hands and fingers. Has increased use of rib and chest muscles, or trunk control. |
Daily tasks: Should be totally independent with all activities. Mobility: A few individuals are capable of limited walking with extensive bracing. This requires extremely high energy and puts stress on the upper body, offering no functional advantage. Can lead to damage of upper joints. |
| T7-T12 | Has added motor function from increased abdominal control. |
Daily tasks: Able to perform unsupported seated activities. Mobility: Same as above. Health care: Has improved cough effectiveness. |
| L1-L5 | Has additional return of motor movement in the hips and knees. |
Mobility: Walking can be a viable function, with the help of specialized leg and ankle braces. Lower levels walk with greater ease with the help of assistive devices. |
| S1-S5 | Depending on level of injury, there are various degrees of return of voluntary bladder, bowel and sexual functions. |
Mobility: Increased ability to walk with fewer or no supportive devices. |
Terms
No two spinal cord injuries are the same. Each person’s spinal cord injury will be the result of a different degree of damage than someone else’s. You may hear the terms “tetraplegia”, “paraplegia”, “complete” and “incomplete” and be given an “ASIA classification” to help grade the type and degree of damage. Following is a description of these terms:
Tetraplegia (or Quadriplegia)
Tetraplegia (or Quadriplegia) is injury or damage to the spinal cord in the cervical region (neck) and will result in partial or complete paralysis of the upper and lower portion of the body. These terms mean exactly the same thing; one has Greek origins and the other Latin.
Paraplegia
Paraplegia is injury to the spinal cord below the neck (T1 or below) and will result in partial or complete paralysis of the lower portion of the body including the legs and sometimes the torso.
A Complete injury
A Complete injury means that, in most cases, messages are unable to travel past the level of injury or there is total blockage of messages. Traditionally, it results in total loss of movement and sensation below the level of lesion. The term “complete” is becoming less commonly used to describe loss of function after spinal cord injury.
An Incomplete injury
An Incomplete injury means there is partial blockage and a degree of movement and/or sensation that can be communicated past the level of lesion. The degree of blockage may be given an “ASIA classification” or be called one of the terms listed under clinical syndromes.
Description of Clinical Syndromes
- Central Cord is an injury to the central cord that usually occurs in the neck and more commonly
affects mobility of the upper limbs - Brown-Sequard is a syndrome that usually results in a larger impairment to one side of the spinal cord and therefore greater loss of movement and sensation to one side of the body
- Anterior Cord refers to “the front” and this type of injury will usually result in impairment to motor
systems with some preservation to sensory systems - Conus Medullaris/Cauda Equina refer to the bundle of nerves (often referred to as the “horse’s tail”) that spread out from the base of the spinal cord. These nerves determine bladder, bowel and sexual function. Damage to the cauda equina may result in partial loss of motor and sensation abilities.
ASIA classification
ASIA classification means that, as well as being determined as complete or incomplete a spinal cord injury may have been classified according to the American Spinal Injury Association (ASIA) as either ASIA A, B, C or D.
The table below explains each classification.
Muscle grading works on a scale of 0 to 5. A grade of 0 indicates no muscle movement and 5 indicates normal muscle contraction against resistance. A muscle grade of 3 means that a muscle is able to contract without any resistance placed on it, but against the force of gravity.
Classification |
Description of Function |
| A = Complete | No motor or sensory function is preserved in the sacral segments S4 – S5 |
| B = Incomplete | Sensory, but not motor function is preserved below the neurological level and includes the sacral segments S4-S5 |
| C = Incomplete | Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3. |
| D = Incomplete | Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more. |
| E = Not Affected | Motor and sensory function are normal |
